RIT, URMC receive grant to study benefits of AI-enabled toilet seat technology
Project expected to enhance patient care toward decreased hospitalizations from heart failure
David Borkholder, the Bausch and Lomb Professor in RIT’s Kate Gleason College of Engineering, is working with the University of Rochester Medical Center to further develop the technological functionality of the FIT Seat.
Toilet seats with high-tech sensors might be the non-invasive technology of the future that could help reduce hospital return rates of individuals with heart disease.
A joint project by researchers at Rochester Institute of Technology and the University of Rochester Medical Center (URMC) will determine if in-home monitoring can successfully record vital signs and reduce risk and costly re-hospitalization rates for people with heart failure. The five-year, $2.9 million venture is funded by the National Institutes of Health (NIH).
A. Sue Weisler
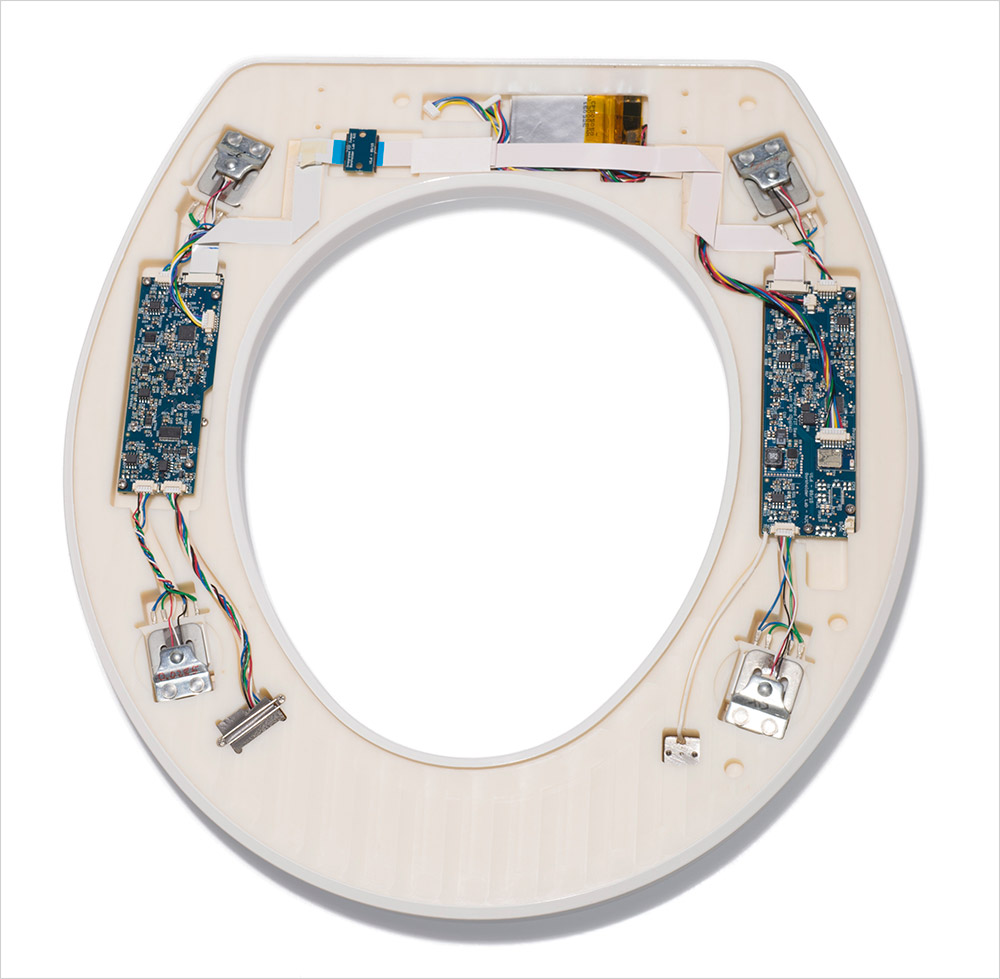
FIT Seat technology embedded in a common toilet seat will generate data regarding a patient’s vital signs. The information will be used to determine if in-home monitoring can successfully monitor vital signs and reduce risk and costly re-hospitalization rates for people with heart failure.
The new Fully-Integrated Toilet Seat, or FIT Seat monitoring system, will incorporate artificial intelligence and improved user interfaces to provide physicians with up-to-date patient data over time and in a format that is easily readable. Artificial intelligence technology will be added as part of an early-alert system to help physicians identify possible deterioration sooner, said David Borkholder, the Bausch and Lomb Professor in RIT’s Kate Gleason College of Engineering. He and Wojciech Zareba, M.D., professor of Medicine, Cardiology, at the University of Rochester Medical Center, will lead a multi-disciplinary research team to further develop the technological functionality of the FIT Seat.
Heart failure is one of the leading causes of adults admitted to hospitals, and more than 6 million adults in the United States have heart disease, according to the American Heart Association. Re-hospitalizations occur in some instances within 30 days to six months of initial treatment. Having a way to intercept these rehospitalizations might afford patients improved care and decrease costs.
“The cost of readmission usually exceeds the cost of the original hospitalization when individuals have a diagnosis of heart failure,” said Borkholder. “We are using machine learning and AI to develop an early alert system so that we can identify when a patient’s health begins to subtly deteriorate and hopefully see it much sooner than the patient would detect it themselves.”
Zareba agreed. “There are a number of factors that can be evaluated in these patients. It is like having a patient on bedside monitoring in an intensive care unit. At home, people don’t usually have these monitoring tools. This seat is serving as a good monitoring tool. Even if it is not continuous, it will be used by patients several times per day, and each time, it will record data and send it to be processed.”
New connections to improve foundational technology
In 2014, Borkholder and Nicholas Conn, a postdoctoral fellow at RIT, developed the original FIT Seat technology, in collaboration with URMC cardiologist Karl Schwarz, M.D. The system provided a robust collection of patient information through what might be considered a non-descript, unassuming instrument. The toilet seat had high-tech sensors embedded on its surfaces that detected heart rates, blood flow, and oxygenation, with the potential to provide near real-time information to physicians about patient status. The seat is now being developed by Heart Health Intelligence.
“The goal is to deploy a system where people with heart failure receive daily medication dosing and other guidance based on FIT measurements of their cardiovascular health, much as people with diabetes use a glucometer to manage their blood sugar,” said Schwarz, who also serves as professor of Medicine and Anesthesiology and Perioperative Medicine at the medical center. He was a key member of the FIT seat development team early on, and notes that the system is a means to help guarantee patient compliance through regular usage.
Using that non-invasive technology as the foundation, the new project launched in summer 2020 with both teams doing the necessary preparations to build the test system, including the data management and user-interface, and to begin recruitment of study-patients.
Sensors in the FIT Seat will measure blood pressure, weight, and heart rate and other key indicators of heart health. The data points will also be unique to each individual involved in the study.
“Individuals have unique features—from distinct eye and hair color to biological characteristics such as an electrocardiogram (ECG),” said Zareba. The sensor algorithm in the FIT Seat is “smart” in that it can be trained to recognize patterns and characteristics that will be distinct to each person, even taking into account the communal nature of the toilet seat in an individual’s home. “Looking at ECG from two people, physicians can see differentiations, so the data on a given patient will not be mixed up.”
A key advance in the FIT monitoring system is the combination of an unobtrusive home monitor with AI technologies and innovative user interfaces for both patients and physicians that will eventually allow for the semi-automated day-to-day management of heart failure and other cardiac diseases. The ability to gather and synthesize data can help physicians identify or predict changes and potentially modify treatment to prevent another hospitalization. Use of AI technologies and the advances in machine learning can speed up the recognition of trends and allow for predictive analysis. Ultimately the overall goal is to demonstrate that the technology is reliable enough to be well-integrated with the health care system.
“One of the key challenges with any technology like this is effective integration into the health care system,” said Borkholder. “Part of what we integrated into the design of the system—and this is where the University of Rochester team is important—we have panel of physicians and advanced practice providers that are going to help us refine the way we present the information so that it is easily digestible. That is key.”
Research expertise
The collaborative effort between RIT and URMC is supported by the NIH’s Multiple Principle Investigators Grants and Funding Program, a research model that is led by more than one principle investigator, often from different organizations, and recognizes the different, necessary areas of expertise. The NIH obligates year-by-year funding and the initial outlay will be $597, 754.
Borkholder will work with Hye Jin Nae, assistant professor in the School of Design in RIT’s College of Art and Design. Her role will be to create user interfaces for both the physicians and the patients. Linwei Wang, professor of computing in RIT’s Golisano College of Computing and Information Sciences, will lead the artificial intelligence aspect of the project. She has an extensive background in the development of algorithms for biomedicine.
Zareba’s URMC team includes cardiologists and research-faculty members: Schwarz; Leway Chen, medical director of the Advanced Heart Failure Program; and Robert Strawderman, chair and Distinguished Professor of Biostatistics and Computational Biology.
“Medicine today is oriented toward prevention; if you have good tools which will allow you to catch certain signs and symptoms that could be worsening, it will be easier to do it. This is the future of medicine,” said Zareba.
Recommended News
-
November 26, 2023
![two American soldiers standing next to each other, one with a rocket launcher on his shoulder. There is debris and heat waves in the air behind them from a recent blast.]()
U.S. Troops Still Train on Weapons With Known Risk of Brain Injury
The New York Times talks to David Borkholder, the Bausch and Lomb Professor in the Department of Electrical and Microelectronic Engineering, about blast exposure.
-
May 27, 2021
![toilet with seat with sensors on it.]()
Smart toilet seat designed to potentially save lives
WHEC-TV talks to David Borkholder, professor in the Kate Gleason College of Engineering and co-founder and head of research and development at Casana.
-
April 28, 2021
![people working on toilet seat prototypes.]()
Alumni join forces to market smart toilet seat
Alumnus Nick Conn’s vision for a one-of-a-kind smart toilet seat that will improve the health of people around the world has made giant leaps toward becoming a reality with the help of one of RIT’s most generous patrons, Austin McChord.
-
February 24, 2021
![two researchers holding toilet seat with sensors embedded on the bottom.]()
Toilet Seat Offers Relief for Heart Patients
ASME.org features David Borkholder, the Bausch and Lomb Professor of Microsystems Engineering, and Nicholas Conn '11, '13 MS (electrical engineering).



